Adult Primary Rhegmatogenous Retinal Detachment Surgery: No Return to the Operating Room Within 90 Days of Surgery
Measure Overview
Use in CMS Programs
- Finalized through rulemaking for inclusion in the Merit-based Incentive Payment System (MIPS) in 2016.
- Implemented in MIPS starting with Performance Year (PY) 2017.
Description
Patients aged 18 years and older who had surgery for primary rhegmatogenous retinal detachment who did not require a return to the operating room within 90 days of surgery.
Measure Specification
Patients who did not return to the operating room within 90 days for complications within the operative eye.
N/A
N/A
Patients aged 18 years or older who had surgery for primary rhegmatogenous retinal detachment.
Surgical procedures that included the use of silicone oil.
N/A
Measure Information
Endorsement History
N/A
Measure Performance in Program
Measure Score by Performance Year
Impact Summary: This measure supports the Merit‑based Incentive Payment System by assessing short‑term surgical outcomes for adults undergoing primary rhegmatogenous retinal detachment surgery, specifically the absence of a return to the operating room within 90 days of the initial procedure.
Performance on this measure is consistently high, with most clinicians achieving rates above 90% and a substantial proportion achieving 100%.
Based on the most recent benchmark data, if clinicians in Deciles 1 through 7 improved to the average performance observed in Decile 8 (100%), the percentage of patients with no return to the operating room within 90 days of surgery could increase by about 5 percentage points, from 94.7% to nearly 100%, potentially improving patient outcomes.
For this measure, Battelle reviewed the following publicly available datasets at Benchmarks - QPP:
- 2026 MIPS Quality Benchmarks.csv (referred to as year 2024 in this assessment)
- 2025 MIPS Quality Benchmarks.csv (referred to as year 2023 in this assessment)
- 2024 MIPS Quality Benchmarks.csv (referred to as year 2022 in this assessment)
- 2023 MIPS Quality Benchmarks.csv (referred to as year 2021 in this assessment)
Battelle analyzed benchmark values for “Measure_ID”=384.
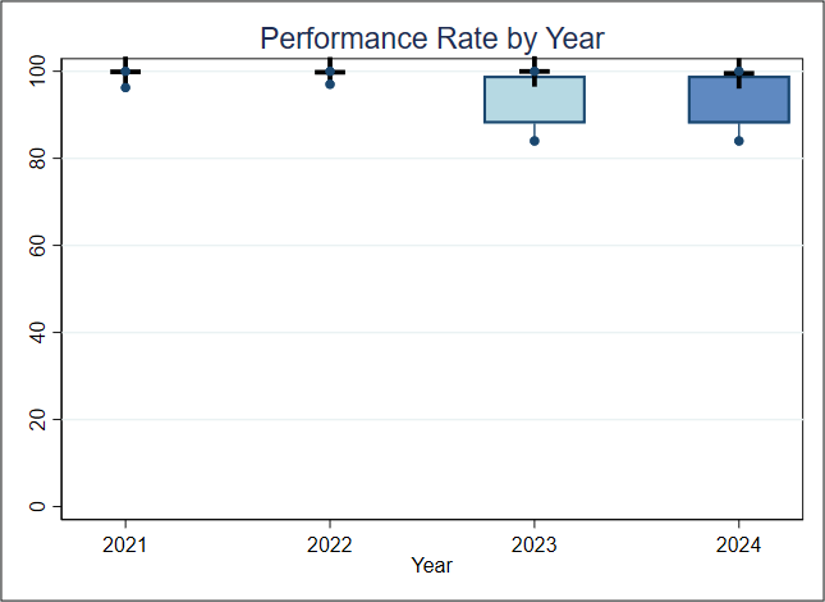
About Figure 1: Figure 1 is a boxplot that shows how rates have changed based on the most recent 4 years of data available. For each year, the boxplot displays a box with lines and dots to help visualize the range and distribution of rates. The dots represent the minimum and maximum rates, and the line connecting them shows the range of the rates. The box itself covers the middle 60% of the rates, from the 20th to the 80th percentile. A “+” sign shows the average rate. This type of graph makes overall trends in rates over time as well as the consistency and spread of the results easier to visualize.
Figure 1. Boxplot of Performance Rate by Year
Figure 1 Interpretation: For each of the 4 years, at least 20% of clinicians have a 100% performance rate and, except for 2022, at least 80% of the clinicians have a performance rate greater than 90%. For this measure, a higher performance rate indicates better quality of care.
Score Distribution for Most Recent Years
About Table 1: Table 1 illustrates the distribution of rates across deciles in the most recent data available.
Table 1. Importance (Decile by Performance Rate, FY2024)
| Mean | Decile 1 | Decile 2 | Decile 3 | Decile 4 | Decile 5 | Decile 6 | Decile 7 | Decile 8 | Decile 9 | Decile 10 | |
| Rate | 94.7 | 71.4-87.1 | 87.1-91.9 | 92.0-93.3 | 93.3-94.7 | 94.7-96.7 | 96.7-97.1 | 97.1-100 | 100 | 100 | 100 |
Table 1 Interpretation: Nearly all clinicians have a rate greater than 80%, more than 80% of clinicians have a rate greater than 90%, and more than 30% of the clinicians have a performance rate of 100%. If the average performance of Decile 8 (100%) is considered a plausible, achievable rate, and the clinicians in Deciles 1 through 7 improved to reach that rate, the estimated percentage of patients with no return to the operating room within 90 days of surgery would go up by about 5% (from 94.7% to nearly 100%), potentially leading to better health outcomes for these patients.
Meaningfulness
Importance
The Meaningfulness criterion will be evaluated as part of the full Preliminary Assessment available in September.
Data Stream Burden Reduction
Data Stream Burden Reduction
This criterion will be evaluated as part of the full Preliminary Assessment available in September.
Alignment with the Patient Health Care Journey
Alignment with the Patient Health Care Journey
This criterion will be evaluated as part of the full Preliminary Assessment available in September.